

The Beginnings (1886-1948)
Glasgow has an important and fascinating history of cancer treatment and research. It began in 1886 with the establishment of the Glasgow Cancer and Skin Hospital at 400 St Vincent Street. After a fundraising appeal, a ten bed hospital was opened at 168, Hill Street, Garnethill, with Dr Hugh Murray as Director. In 1893 the Directors decided to limit the work to the treatment of cancer patients only, and appointed a full staff of medical officers, including a pathologist. This was the first hospital in Scotland to deal solely with cancer patients. There was an outdoor dispensary at 22 West Graham Street, and a domiciliary nursing service was established to assist patients in their own homes. This was 60 years before the establishment of the Marie Curie Foundation.
The Director of the new Glasgow Cancer Hospital was Dr George Beatson (later Sir George), a major pioneer of cancer treatment. He published a paper in the Lancet in 1896 of three cases of women with breast cancer, in which their ovaries were removed, with significant improvement in outcome. This remains one of the most significant advances in cancer treatment.

Following a further appeal in 1896, the Glasgow Cancer Hospital moved to larger premises at 132-138 Hill Street, where two buildings on the site were converted into a modern 30 bed hospital with provision for the pathological study of cancer. Following a further appeal in 1906, a research department was established within the hospital and this was opened in 1912 by Her Royal Highness Princess Louise, Duchess of Argyll.
At that time, it was announced that his Majesty King George V wished it to be called The Glasgow Cancer Hospital. Analysis of the admissions between 1894 and 1922 showed that people from 22 out of the 35 Scottish counties had availed themselves of the hospital services as had a number of people from England and the Dominions of the then British Empire.
In 1921, a new symmetrical X-Ray Apparatus (165,000 volts) costing £872 was installed in the Cancer Hospital. Some treatments took up to 8 hours. In 1928, Lady William Burrell generously donated £10,000 to allow Sir George Beatson to purchase a supply of Radium needles. At that time, there was very little Radium - approximately half a gram - available in Glasgow for the treatment of cancer, and this purchase allowed the development of this technique.
In 1930, the Radium Institute was inaugurated by Principal Rait of the University of Glasgow. The Institute was allocated 14 beds and two single rooms. Arrangements were made to admit patients referred from across Glasgow, also Paisley and Greenock. Dr. R R Morrison was appointed as the first Radium Medical Officer. The Institute became the nucleus of the present Beatson Cancer Centre.
In 1932, Dr. Peacock, previously Director of Research (1928) of the Hospital, was appointed as the Administrative Medical Officer, succeeding Beatson. In 1933, the X-Ray machine was replaced by a new, more powerful (200 to 400 kV) apparatus costing £1540. At this time, a Radiographer was appointed to the Hospital.
In the mid-1930’s, Radium therapy could be received at other hospitals – the Royal Samaritan, Victoria Infirmary, Greenock, Glasgow Royal Infirmary, and the Ear Nose and Throat Hospital. The Glasgow Royal Cancer Hospital “lent” or hired out sources to these hospitals. This facility was stopped at the start of World War II, as radium sources had to be securely stored to ensure they were not damaged by aerial bombing. Special underground safes were constructed to store the sources when they were not in use.
Professor Ken Calman and Dr Gerry Robertson
Radiotherapy

When the National Health Service was set up in 1948, the treatment of cancer patients in Glasgow and the surrounding areas was well established. Radiotherapy was, however, still a very minor specialty.
At that time, there were four sites where radiotherapy treatment could be delivered:
- the Southern General Hospital,
- Glasgow Royal Cancer Hospital,
- the Western Infirmary
- the Royal Infirmary
Southern General Hospital
There was a radiation theatre at the Southern General Hospital / David Elder Infirmary (1938 -1952) where radium implants could be carried out. Patients with tumours at a variety of sites - breast, uterus, cervix, head and neck, larynx, skin, lung, and a few other areas, were able to be treated with this technique with varying success.
The Unit was closed in 1952 as a result of concerns about radiation protection.

In 1948, radiotherapy treatments in the Glasgow Royal Cancer Hospital, while "state of the art", were still primitive by present day standards. Gynaecological tumours were treated with Caesium packs, inserted manually. Some superficial tumours were treated with Caesium needle implants, or 100 kV X-ray beams delivered from a radiotherapy machine. Deeper sited tumours could be treated using 250 kV beams.
In 1952, the Glasgow Royal Cancer Hospital was renamed the Royal Beatson Memorial Hospital.
Western Infirmary
At the Western Infirmary, a single Department of Radiology and Radiotherapy had been established in 1930 under the direction of Dr Stanley Scott Park. The Radiotherapy section contained a Superficial X-ray treatment (XRT) room, a high voltage Deep XRT room, and a special Radium room. A separate Radiotherapy Department at Glasgow Western was established in 1946. Dr Park remained the director of the Radiology Department.
Dr Alex Charteris was appointed Director of Radiotherapy of the newly formed Department of Radiotherapy (1946). He had previously been the Donald Research Scholar for Cancer (appointed 1928) and had worked as a Radium Therapist at the Glasgow Royal Cancer Hospital. He continued to be in charge of the Royal Cancer Hospital as well as the new Radiotherapy Department at the Western Infirmary. The two Radiotherapy departments functioned as a single unit. Dr Charteris was joined by Dr T Martin Scott. In 1948, the department at the Western Infirmary had a good supply of Radium needles (the Unit had been recognised as one of four National Radium Centres in Scotland in 1930) and a Radium Beam Unit (installed in 1938). The Unit acquired two Deep X-ray machines, one superficial machine and one Strontium 90 unit. Subsequently Dr Charteris obtained a unit with a stronger source of Cobalt, and eventually a new Cobalt machine.
In 1957, the Western Regional Hospital Board decided that it wanted to develop complementary Radiotherapy units at the Western Infirmary and at Glasgow Royal infirmary. A self contained Department of Radiotherapy (48 beds) was built at the Western Infirmary. In 1962, the first linear accelerator (Linac) was installed. The new department was opened in 1963, four months before Dr Charteris retired. The Department eventually had 6 Linacs - 3 Elekta SL75-5 Linacs, 2 Varian CL600 C Linacs, and 1 Varian CL2100 C. There were 2 Kilovoltage machines and 2 simulators.
Glasgow Royal Infirmary / Belvidere Hospital
In 1948, Glasgow Royal Infirmary had a small Radiotherapy section of the Radiology department. Dr RR Morrison was the consultant radiotherapist. In 1947, the Radium Commission visited the Infirmary - a designated Radium Centre - to assess the Radiotherapy facilities. It recommended an increase in accommodation, installation of two deep X-ray therapy units, and the appointment of an assistant to Dr Morrison. Two 250 Victor X-Ray Therapy units were installed in a waiting room in the south wing of the outpatient department. The walls of the room were covered with lead or Barium plaster to protect patients and staff in the vicinity.

By 1954, Dr Morrison had two assistants, Dr J C Davidson and Dr J M Glennie. In 1955, the Radiotherapy department was moved from the outpatient department to the Gate House. Dr Morrison requested that Radiotherapy facilities needed to be expanded, and it was agreed by relevant Boards that the new site would be at Belvidere Hospital.
Fifty six beds were allocated for inpatient care. In 1959, the Department of Health authorised the building of a new Radiotherapy Department, which became functional in 1963. A Linac and a Cobalt machine were installed. The number of machines was increased over the years, with the installation of two Vickers Linacs, later replaced by a Philips SL75 (1978) and an RDL Dynaray (1981). The Department also had two Kilovoltage machines and a Simulator.

The Glasgow Institute of Radiotherapeutics
In 1965, the Units at the Western Infirmary and Belvidere Hospital were amalgamated under single management, known as the Glasgow Institute of Radiotherapeutics. The new Institute had clinics in Stirling, Falkirk, Ballochmyle, Paisley, Oban, Inverclyde and Dunoon. Dr Keith E Halnan was appointed as the Medical Director, and Dr Stewart Orr, a Physicist in the Regional Physics Department, was attached to Belvedere. In collaboration with Dr Halnan, he developed equipment to determine dose distribution, and worked on the technology of x-ray diagnosis and radiotherapy.
Dr Halnan and Dr John Lenihan (Director of the Glasgow Regional Department of Clinical Physics and Bio-Engineering) introduced research into Neutron therapy. The Neutron generator installed at Belvidere was one of two installed in the UK; the other unit was sited in the Christie Hospital, Manchester. The project, started in 1967, was led by Dr Bob Lawson. He and Dr Orr performed much important background research. The Neutron therapy Unit started in 1971. About six patients were treated before the project was discontinued in 1978, due to the unreliability of the machine. They also investigated the diagnosis and treatment of cancer using radioactive isotopes. Professor Tony Nias, who was carrying out research into radiation biology, also collaborated in the neutron project.
This research was of value to the clinicians in the Hammersmith Hospital, London who were also treating patients with neutrons. The research also helped establish Glasgow as a major centre for experimental radiotherapy research in the UK.
Clinical Research and Developments
The Glasgow Cancer Hospital research laboratories were established under Sir George Beatson’s directorship in 1920. Its Cancer Research Department had a major boost by the appointment of Professor John Paul to the post of Director in 1966. Professor Paul had been based in the University Department of Biochemistry since 1954, with a personal Chair in Cellular Biochemistry conferred in 1964. The research laboratories were further expanded and renamed the Beatson Institute for Cancer Research in 1967. With the agreement of the University and support from the Wolfson Foundation and the Cancer Research Campaign, a new site for the Institute was opened at Garscube in 1976.
In 1965, Dr Halnan was involved in the establishment of the Department of Radiation Biology, under the leadership of Dr A H W Nias (Consultant Medical Radiation Biologist), later Professor Nias (1972-1977). He was associated with the neutron project and hyperbaric oxygen studies, as well as developing the Department of Radiation Biology. He was also interested in platinum coordination complexes as chemotherapy agents and radiation sensitisers. Professor Nias was succeeded by Professor James Kirk (1977-1983) who had an interest in developing mathematical models to allow the comparison of different radiation doses (Radiation Biological Effect). He died in 1983 and was succeeded by Dr (later Professor) Tom Wheldon from the Hammersmith Hospital (1983-2000), who had similar interests.
The Academic Department of Radiation Oncology was set up in 1980 with the appointment of Professor Ann Barrett (1986-2001). Professor Barrett was interested in the treatment of paediatric tumours. She was later joined by Professor Roy Rampling (1987-2010) and subsequently by Professor Anthony Chalmers (2010 - current). The latter two researchers had a strong interest in the treatment of brain tumours.
Within the Glasgow Institute of Therapeutics there were other major clinical research and development projects. Dr Eric R Watson worked in association with the MRC in investigating the value of exposing gynaecological patients receiving XRT to hyperbaric oxygen. He was also involved in assessing the value of administering radiation sensitisers to patients receiving XRT. Drs E R Watson and M A C Cowell set up a large retrospective gynaecology data base from in house case sheets. This large analysis was the basis of future very successful in house studies combining XRT and chemotherapy to treat gynaecological tumours.
Dr Gerry Robertson carried out an analysis of the treatment of laryngeal tumours in house, which led to the rationalisation of the radiotherapy regimen used. With the assistance of the Royal College of Radiologists, he then led a UK national survey of radiotherapy treatment of laryngeal cancer. This identified that unplanned breaks in therapy reduced the efficacy of treatment. Efforts have been made to stop this practice across the UK.
Three dimensional Radiotherapy planning was introduced in the early 1990s and the Beatson Oncology Centre was one of the first centres in the UK to adopt the 3-D HELAX planning system. This improved the accuracy of treatment planning.
Chemotherapy treatment was widely adopted in the Institute in the early 1970s; and the name of the Institute changed to the Glasgow Institute of Radiotherapy and Oncology.
In the late 1970s, under the leadership of Drs Fiona Cameron and Michael Willoughby (consultant paediatric haematologist at Royal Hospital for Sick Children), Total Body Irradiation (TBI) was introduced as preconditioning for children with acute leukaemia receiving a bone marrow transplant. This service was later expanded by Dr Gerry Robertson and Dr Alan Burnett (consultant haematologist at Glasgow Royal Infirmary) to treat adults receiving a bone marrow transplant as therapy for Acute Myeloid Leukaemia.
1980 saw the Introduction of automated intracavitary therapy- after loading- at the Western Infirmary, and later at Belvidere Hospital.
In the early 1980s there were about 12 Consultant Clinical Oncologists treating patients with both chemotherapy and radiotherapy. There was a small Gynaecology team (Dr M A C Cowell and Dr E R Watson) in the Western Infirmary Unit; the remaining consultants were "generalists". At that time the Royal College of Radiologists recommended that Clinical Oncologists should cease being generalists and only manage patients with tumours arising at 2 or 3 anatomical sites. This practice was introduced into Glasgow. This change in practice led to marked improvement in patient management. Tumour specific teams were established. They contained nurses, radiographers and dietitians, and eventually Clinical Nurse Specialists (CNS). These CNSs had a specific interest in the management and support of patients with tumours arising at certain anatomical sites.
Radiation Oncologists/Clinical Oncologists had always been aware of the side effects associated with radiotherapy, such as radiation dermatitis, nausea, diarrhoea and dry mouth. From 1960 onwards, there was a small General Reaction Clinic run in the three Radiation units. The site-specific CNSs helped establish Reaction Clinics for patients treated by their team. They helped identify more subtle side effects arising in their patients and instigated the establishment of Chronic Side Effect Clinics for the many patients cured of their cancers who have to live with permanent side effects. Counselling services were also introduced.
The establishment of site specialisation also stimulated the establishment of multi-disciplinary teams - Medical Oncologists, Clinical Oncologists, Surgeons, Nurses, Dieticians, Radiologists, Radiographers and Pathologists. These met weekly, discussed all patients’ data, and decided jointly on the best management for each patient. Overall, the introduction of Site Specialisation and the development of new therapies and treatment techniques have improved patient survival and quality of life.
In the 1990s, following the setting up of the Gynaecological Data base, Professor Stan Kaye and Dr Symonds led a number of MRC trials to assess the value of combined Chemotherapy and Radiotherapy in the management of patients with various gynaecological tumours. These were very successful and determined future research and treatment of patients with these cancers.
In 1988, the Royal Beatson Memorial Hospital was finally closed, and patients were treated at the Western Infirmary Unit. In the same year, the Department of Medical Oncology was merged with the Glasgow Institute of Radiotherapy and Oncology, and also moved into the Western Infirmary Unit.
In 1996, the Radiotherapy department at Belvidere was closed. All patients were moved to the Unit at the Western Infirmary. As a result of the "Centralisation" of Oncology services and the merger with the Medical Oncology department, the Unit was renamed the Beatson Oncology Centre (BOC).
In the 1990s, the Scottish Office finally recognised that the Linac availability in the West of Scotland was suboptimal. Funding was allocated to build a state of the art Radiotherapy Satellite Centre at Gartnavel Hospital. Five Linacs were installed, and the satellite was opened in 2002. In the late 1990s the Scottish Parliament also finally recognised that the Hospital and Radiotherapy facilities available at the Beatson Oncology Centre were totally inadequate.

A new unit with state of the art equipment, inpatient and outpatient facilities was built at Gartnavel Hospital, incorporating the previously built satellite. The new unit, named the Beatson West of Scotland Cancer Centre (BCC), was opened on February 2008.
Despite the logistical difficulties, the Beatson Medical and Physics staff continued to develop treatment techniques to endeavour to provide top of the range therapy. In the 1990s, Computerised Tomography (CT) planning was introduced. This improved the accuracy of covering the tumour tissue present at the site being treated, which theoretically should improve response rates.
Intensity Modulated Radiotherapy Treatment (IMRT) was introduced into Glasgow in 2005. Glasgow was one of the first centres in the UK to offer this treatment. This technique - a great step forward in the delivery of radiotherapy treatment - allows linear accelerators to be used to safely deliver precise radiation doses to a tumour, while minimising the dose to surrounding normal tissue. This should reduce the acute and chronic side effects of therapy and greatly improve patients' quality of life.
VMAT/RAPIDARC, an advanced version of IMRT, was introduced into the BCC in 2010. This allowed patients to be treated accurately by IMRT, and the treatment time was greatly reduced improving the efficiency of Linac use.
Since the 1990s the number of Radiotherapists working in the BCC has increased dramatically, there now being about 50.
The Beatson West of Scotland Cancer Centre
The new Beatson West of Scotland Cancer Centre opened its doors in 2007 and delivers an unprecedented level of care to thousands of patients from across the West of Scotland.
The £105 million state-of-the-art facility is the leading centre for delivering non-surgical cancer care in the West of Scotland. It rivals Europe’s top cancer hospitals in terms of facilities and equipment. The Beatson provides West of Scotland cancer patients and staff with the most cutting edge equipment, treatments and surroundings to fight cancer.
Serving a population of 2.6million – more than half the Scottish population – the centre has clinical links with 21 hospitals in the West of Scotland.
Beatson cancer specialists provide clinics at:
- Ayr and Crosshouse Hospitals, Larbert Hospital
- Glasgow Royal Infirmary
- Royal Alexandra Hospital in Paisley
- Wishaw General Hospital, Monklands Hospital
- Hairmyres Hospital, Vale of Leven Hospital
- Inverclyde Royal Hospital, Victoria Infirmary
- Lorn and Isles District General Hospital.
It is Scotland’s biggest cancer centre, and the second largest in the UK. More than 8,000 new patients are seen at the Beatson every year.
To help meet this future demand, work was carried out to develop plans for a West of Scotland Satellite. Following a detailed assessment, which took into account a wide range of factors such as travel times, clinical benefits and site requirements, Monklands Hospital in Airdrie was confirmed as the preferred location for the new Centre which is called The Lanarkshire Beatson. It opened in 2015. This Centre operates as a satellite facility for the Beatson West of Scotland Cancer Centre in Glasgow, increasing access to the state-of-the-art radiotherapy treatments and allows many more patients in the West of Scotland to be treated closer to home.
It is equipped with the most advanced technology to deliver the same world-class treatment and techniques currently provided at the Glasgow centre. There are two new state-of-the-art linear accelerators, which deliver high-energy radiation to shrink tumours and kill cancer cells, with expansion space for a third machine, if required. The Centre also has a CT simulator to help plan radiotherapy treatment. This enables around 80 patients a day who require radiotherapy for lung, breast, prostate and rectal cancers to attend for therapy.
Dr Gerry Robertson
Surgery
Surgical removal of a localised cancer remains the traditional first approach to treatment for many cancers. From 1948 there was increasing use of endoscopic removal instead of open surgery.
Specialised surgery was performed for
- gastrointestinal and urological cancer, initially by general (abdominal) surgeons then by specialist gastrointestinal surgeons and urological surgeons (see surgery and urology)
- gynaecological cancers by gynaecologists
- thoracic cancers by thoracic surgeons
- brain cancers by neurosurgeons
- eye cancers by ophthalmologists
- ear, nose and throat cancers by otorhinolaryngologists
- skin cancers by dermatologists and plastic surgeons
- bone cancers by orthopaedic surgeons.
Medical Oncology
1974-1985

During the 1960s and 1970s, much clinical and research work in cancer continued across Glasgow in surgery, medicine, radiotherapy, haematology, gynaecology and paediatrics. During this time, a new specialty emerged, that of medical oncology, focusing particularly on chemotherapy, hormone therapy and immunotherapy.
The major Cancer Charities invested in this across the UK, and the University of Glasgow was fortunate to receive a major Cancer Research Campaign grant in 1973 to establish a chair, clinical facilities and research laboratories. Kenneth Calman was appointed professor and the Department began in October 1974. This was the first Medical Oncology Department in Scotland.
The Department of Oncology
Its beginning was not without difficulty: no staff, no beds, no offices and no research space. A secretary was appointed, and a room was found in the Nurses home as an office. Clinical facilities became available in the Professorial Medical Unit (Professor Sir Abraham Goldberg) at the Western Infirmary (find out more). Dr Gordon McVie was appointed senior lecturer, and Dr Mike Soukop as senior registrar, and the work began. Patients began to be referred to the Unit, though an analysis showed that 60% of patients referred in the first 6 months died in a month without treatment because of their very late referral. This is similar to other new specialties in their first few months. The unit also developed an interest in Palliative Care at this time.
An annual Report was published each year and the notes which follow are expanded in these Reports. The Unit moved to Ward 7B at Gartnavel General Hospital in 1977 and at last had a place to care for patients and their families. The Department had no offices, but some small offices were placed between the lifts for receptionists in the corridor, who refused to use them. The professor took one!
The Department developed a logo, designed by a very special patient, Professor Alexander John Haddow (see Infectious Diseases). He was a Fellow of the Royal Society and had worked in Africa for many years and was involved in the discovery of Burkitt’s Lymphoma and the Zika virus (find out more).
The Logo was a four pointed Celtic knot symbolising the interaction of the four main cancer treatments at the time, namely surgery, radiotherapy, chemotherapy, and hormone therapy, bound together with the “O” for oncology.
Laboratories became available in 1975 in a large house in Horselethill Road, not far from the hospital. They were formally opened in 1976 by the Principal Sir Alwyn Williams and Professor John Lajtha from the Paterson Laboratories Manchester, representing the Cancer Research Campaign. The Department was joined by Dr John Durham and Dr Ian Freshney, who had been at the Beatson Institute.
The Head of the Beatson Institute, Professor John Paul, and Professor Calman, wrote a short book together - An Introduction to Cancer Medicine (MacMillan Press Limited 1978).

The clinical side began to develop and more and more patients were being referred. Clinics were also established in Ballochmyle Hospital in Mauchline in Ayrshire, and Inverclyde Hospital in Greenock. From this was established a wide range of clinical groups involving clinicians from across the West of Scotland. These were generally chaired by staff from outside the Department, and there were strong links with radiotherapy and haematology. From these early beginnings, a Clinical Trials Secretariat was established to progress this work. These included effective links with Radiotherapy, Surgery, Gynaecology, Urology, Haematology, Sarcomas and Dermatology. Patients were being entered into over 15 trials covering a wide range of conditions, many developing the use of new drugs.
Staff numbers were also expanding and when Dr Gordon McVie went to a post in Amsterdam, Dr Stanley Kaye became the new Senior Lecturer in 1980. This was a time of real change in the development of new drugs for cancer. One of the most exciting was Platinum for use especially with testicular cancer, and from a disease which was almost untreatable to one in which long-term remissions and cures became possible. This was breath taking. The use of multiple drugs, new regimes and new drugs made medical oncology a very exciting specialty of which to be part. The clinical trials part of the work expanded and developed, and became an important force for change.
One of the most important aspects of the work of the Department was the international dimension and to learn from those at the forefront of change. This was done by attending a wide range of meetings but also in two other ways.
- The first was that Professor Calman was awarded the Hutton MacConnachy Travelling Fellowship by the Royal College of Physicians and Surgeons in Glasgow in 1974. This was right at the creation of the Department and various places in New York and Boston were visited, and this proved to be very valuable.
- The second aspect was the visitation to Glasgow of several distinguished cancer specialists.
- The first was Professor Lucien Israels from Paris. He had several special interests, including immunotherapy and taught the Department many things.
- The second was Professor Philip Schein from the National Cancer Institute in Bethesda Maryland and the Vincent T Lombardi Cancer Centre. He provided significant scientific and pharmacological expertise.
- The third was Professor Paul Carbone, based in the University of Wisconsin, and who also ran the Eastern Cooperative Oncology Group, a multicentre clinical trials group. The Department joined this, and was able to put Glasgow patients into some of the leading edge clinical cancer trials in the world. Each of these individuals, and others, kept the Department at the forefront of research and patient care.
The “Team Approach” was central to the work of the Department; medical and nursing staff, dieticians, physiotherapists, pharmacists, pathologists and a psychological interest were all integrated into the care of patients. Before clinics, for example, the team sat down and went through the notes of the patients coming to the clinic, and noted which staff members were most appropriate to see the patient. It might be the professor or the medical staff, but equally it might be the dietician. This was patient focused care.
A Course was established at the University entitled Basic Principles of Cancer Chemotherapy. This began in 1978 and lasted for a number of years. A textbook was written with the same name and co-authored by Professor John Smyth, then in Edinburgh, and Professor Martin Tattersall in the University of Sydney, Australia. The Foreword was written by Professor Whitehouse from Southampton University. It was an important initiative, and allowed staff to meet new people and new ideas.
Research
Research was at the heart of the work of the department from palliative care, the development of new drugs, patient and public education to a wide range of studies in the biological sciences. In many of these, there was collaboration with other Universities and in Drug Development, the link with the University of Strathclyde Department of Pharmacy, was particularly important.
As examples, here are a few from the 1982-3 Annual Report. There was a major interest in nutrition and metabolism in cancer patients in order to understand the mechanism of cachexia. Pharmacokinetics and pharmacological aspects of cytotoxic drugs featured large, as did drug formulation. There was a special interest in drug resistance and there was a large group of products studied in this area. There was a wide range of research projects relating to tumour biology and tumour products. This produced 28 publications and a range of presentations at scientific meetings, conferences and teaching engagements.
Patient and public involvement and education
At the heart of patient care is the patient, his or her family and friends and the wider public. Over the first 10 years of the establishment of the Department, this was a priority and was developed in a series of ways.
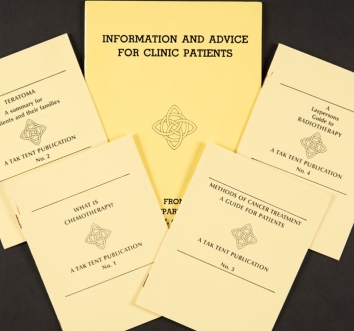
At the simplest level, this was in the production of a series of leaflets for patients on a wide variety of subjects. Patients themselves were involved in their writing using their experience to help others. As a good example of this, the booklet written on how to get illness benefits was written by a patient who worked in a Benefits Office. These booklets provided a range of information on topics such as the working of the clinic, the staff involved, i.e. nurses, pharmacists, etc and ongoing patient support. There were booklets on guides to chemotherapy and to radiotherapy, and on specific conditions such as Teratoma. One booklet entitled “We can Help” was about diet and how to eat well in which recipes were provided for patients. Finally, there was a short booklet on how to set up a Tak Tent Group. In each of these, patients and their families were involved in writing them.

This led to the establishment of a series of public lectures in Glasgow on cancer, its causes and treatments. They were attended by several hundred people and a small booklet “Living with Cancer” was produced for the wider public. One of the most significant developments was the establishment of Tak Tent, the old Scots phrase for Take Care. A series of groups developed which helped patients and families support each other and learn from each other. It began in the home of Professor Calman where there was recognition that patients could teach professional staff a great deal.
This then became a regular meeting at the hospital with a talk by a member of staff followed by refreshments and general meeting. This resulted in the setting up of over 30 groups, locally based, who met to support each other. They taught the staff much over the years. Tak Tent has changed and is now Cancer Support Scotland, based in Glasgow in a beautifully renovated Arts and Crafts Chapel in the grounds of Gartnavel Royal Hospital - and the work continues.
Perhaps the most profound effect of these experiences was the impact on staff, who learned so much from patients. This included our scientific staff, who met patients and recognised their research was for real people with cancer.
Professor Calman has described this as the most important learning experience of his clinical career.
The other novel aspect of this work was on patient and public education, and the public lectures have already been noted. An education Group was set up under the direction of Ann Calman and this incorporated the development of educational material for medical students, nurses and other health professionals. This included videos of conversations with patients which could be used for teaching purposes. The Department was assisted in this by Professor Jan McDonald, who was Professor of Drama at the University. It should be remembered that this was in the late 1970s when not much of this kind of material was available. The nurse teaching programmes were at the leading edge of nurse education.
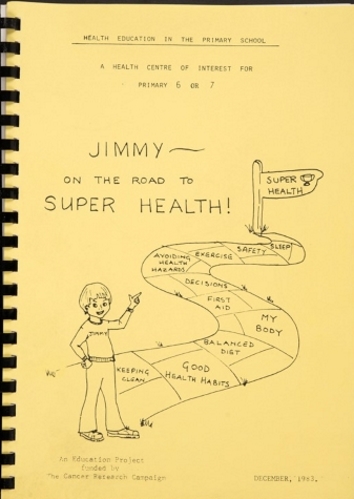
Finally, and of special interest, was the programme developed for the improvement of the health of children at primary school level. This programme, Jimmy on the road to super health, was introduced into over 50 primary schools in the West of Scotland and Northern Ireland. It used a curriculum-based approach and was an early attempt to change health behaviour in children. It was a real first, in particular aiming to prevent the uptake of smoking. A significant range of material was generated and the Education Group pioneered the programmes now available.
In retrospect, there are a number of things which seem important.
The Department helped to build a new specialty, laying the foundations, and building the links and collaborations for further development in Glasgow and beyond.
Here was the beginning of the integration of clinical trials work and patient involvement in action in Tak Tent, which demonstrated the power of the patients’ experience and their real courage and wish to help others.
The broader educational programmes were at the leading edge and the schools programme was almost unique.
The final aspect of this was to watch the progress of staff, who were part of the Department, going on to achieve great things in their own professional area.
Professor Calman stepped down in 1984 to become Dean of Postgraduate Medicine at the University and a consultant in Palliative Care at the Victoria Infirmary Glasgow.
Professor Ken Calman
1985-2002

In 1985, Professor Stan Kaye was appointed to succeed Ken Calman and the Department of Medical Oncology continued to operate from two sites – clinical facilities on the 7th floor of Gartnavel General, with the laboratories less than a mile away at No. 1 Horselethill Road.
For both of these activities, a priority at that time was to move towards greater integration with relevant colleagues in the Hospital and University and this was achieved in three steps:
-
In 1986, Ann Barrett was appointed to the University’s first Chair of Radiation Oncology, the Cancer Research Campaign Chair having been renamed Medical Oncology. This partnership was important in demonstrating the greater integration of the two non-surgical specialities dealing with the treatment of cancer patients in Glasgow. This extended to teaching (a joint MSc course in oncology was created) as well as to research and therapy, and also incorporated the Department of Medical Oncology led by Dr Mike Soukop at Glasgow Royal Infirmary
-
In 1988 the Department of Medical Oncology merged its clinical facilities with those of Radiation Oncology to form an integrated cancer treatment centre at the Western Infirmary under the title Beatson Oncology Centre. This was recognised as the largest cancer treatment centre in Scotland, responsible for a population of around 2.8 million. It was one of the first in the UK to introduce multidisciplinary meetings and clinics, bringing surgical colleagues (e.g. Professors David George, Rona Mackie and Tim Cooke) into tumour-specific teams with all the advantages of specialist groups
-
In 1990, the laboratories of the Department of Medical Oncology (together with those of the Department of Radiation Oncology) moved to refurbished facilities at Garscube (the Alexander Stone Building) which were adjacent to and linked with the Beatson Institute of Cancer Research. This is the largest cancer research institute in Scotland; it was fully supported by the Cancer Research Campaign, and with enthusiastic input from successive Institute Directors, John Paul and John Wyke, this ensured that integration of research with the Department of Medical Oncology was made feasible. A priority was to appoint first class scientists to spearhead collaboration between the Department and the Beatson Institute, and as successive Directors of Laboratory Research, Paul Workman (1991-1993), Allan Balmain (1993-1996) and Bob Brown (1996 – 2002) were key to the developing programme of translational research, particularly in the fields of experimental therapy and drug resistance.
Highlights of this research included the expansion of clinical trial activities, particularly those focusing on early clinical studies of anti-cancer therapy, as well as anti-emetics. A total of 27 studies were completed and published.
Professor Kaye left Glasgow in 2000 to take up the Chair in Medicine at the Institute of Cancer Research in London. ") Professor Stan Kaye
Professor Stan Kaye
2002-2011
In 2002, Professor Jim Cassidy was appointed to succeed Stan Kaye. Professor Cassidy was returning to Glasgow after 9 years as the foundation holder of the chair of oncology at Aberdeen University.
The department then had some turnover in senior staff. Chris Twelves and Ann Barrett left in 2003, Rob Jones was recruited from Astra Zeneca as a new Senior Lecturer in Medical Oncology, and Paul Vasey was appointed as Director of the CRUK trials unit.
Several opportunities to advance medical oncology presented themselves and initiatives were put in place to consolidate the national and international standing of the department. These concentrated on four main areas;
- Taking advantage of the centralized nature of specialist oncology services to enable clinical research in the solid cancers that commonly occur in the Scottish population
- Connecting and collaborating with the world class basic research in the Beatson Institute
- Engaging more fully with Glasgow University departments and facilities to enhance Glasgow cancer research more generally
- Reaching out to other centres in UK and internationally to foster research with global impact
The following is a non exhaustive list of such initiatives and highlights within each area which interlock to describe the developments over the decade.
- Non surgical oncology practice was spread over 4 hospitals (Western Infirmary, Gartnavel Hospital, Glasgow Royal Infirmary and Stobhill Hospital). Each hospital also serviced a number of satellite clinics, often supported by a mix of Medical Oncology and /or Clinical Oncology personnel. A commitment was made by the Scottish Government to a new purpose built cancer hospital on the Gartnavel campus. This opened in 2007 and contained state of the art clinical facilities and radiotherapy machines. The new Beatson Oncology Centre serves 60% of the Scottish population or some 2.8 million people. This presented huge potential to increase trial recruitment across all cancer types.
- This was also the era in which multidisciplinary team working became a pre-requisite for cancer centre designation and accreditation. Glasgow had something of a head start in this regard with this mode of working already in full swing for some tumour types, especially those which had been traditional areas for research such as ovarian, breast and testicular cancers. It was apparent that major changes would be required to extend this way of working across all cancers. In close collaboration with the NHS, University of Glasgow and the Post-graduate Deanery, academic clinical fellows were introduced into the various other disease teams with a specific remit to encourage trial recruitment, whilst ensuring that trainees had exposure to all major tumour types in their training.
- The Cancer Research UK trials unit was led initially by Paul Vasey until his departure to Australia in 2004. The strength of the unit was confirmed by an Alpha star rating at the review and quinquennial grant renewal. On Paul’s departure, Prof Cassidy then took over the Directorship and was awarded grants from the Scottish Government and the NHS to found the Scottish Clinical Trials Network (SCTN). Glasgow became the hub of this organization as CACTUS (Cancer Clinical Trials Unit for Scotland). This enabled us to cast the net even wider for trial participation and also allowed us to develop core expertise in trial design, statistics and operational logistics.
- Whilst links with the Beatson Institute had been established over many years, the arrival of Professor Karen Vousden (read more) as the Director of the Institute in 2003 served as a catalyst for more integration of the basic research within the department. This was cemented by clinical training fellows in Medical Oncology taking time out of their curriculum to fill some of the Institute PhD positions. Further testament to this integration was the appointment of Jeff Evans to a group leader position in the Institute when he was awarded a personal Chair by the University of Glasgow as Professor of Translational Cancer Therapeutics.
- Professor Bob Brown, who had been Laboratory Director of research, departed in 2007 and was replaced in the first truly jointly funded senior post by Prof Peter Adams, who continued working on the theme of epigenetic regulation of cancer which had been established for several years in Glasgow by Bob.
- The first NHS Medical Director of the Beatson West of Scotland Cancer Centre was Alan Rodger. He was an ardent supporter of the trials unit and was instrumental in securing accommodation for the unit including day patient beds, lab space and office accommodation in the basement floor, which was a far cry from the days of a tiny single office between the lift shafts at old Gartnavel! Since Haemato-oncology was in the same building, it made sense to integrate it into the trials activity. Very soon we were running 100 plus studies per annum, and reviewing 3-5 new protocols per week. These were composed of a mixture of pharmaceutical sponsored and local investigator led studies, as well as trials hosted for other CRUK units as our national and international reputation increased. Trial recruitment peaked out at some 15% of all patients referred to the Beatson Oncology Centre being enrolled in therapy studies of one sort or another. A major highlight was the SCOT study (Short Course Oncology Therapy) which was a large randomized trial of 3 versus 6 months of post operative chemotherapy in colorectal cancer patients. This recruited close to 4000 patients and forms the cornerstone study on a multi national consortium effort (IDDEA) to definitively answer this practice changing question. Long term follow up is still going on for this study.
- As part of a UK wide initiative to strengthen research infrastructure, Glasgow competed for and won the designation as an Experimental Cancer Medicine Centre (ECMC) and thereafter also became a CRUK designated Key Clinical Centre. This secured Glasgow’s position as a hub for clinical and translational cancer research which it maintains to the present day.
These studies included the first clinical trials of various drugs which have gone on to become standards of care, including the antiemetic, granisetron (Cassidy et al, 1988) and the chemotherapeutic agents, capecitabine (McKean et al 1998), docetaxel (Bissett et al, 1993) and pemetrexed (McDonald et al 1998). Detailed in-house pharmacological studies were a hallmark of these trials, with invaluable technical help from Bob Blackie, Albert Setanoians and Jeff Cummings.
Other key research areas reflected the interests of the Laboratory Directors; these included aspects of hypoxia and drug development (Paul Workman) and molecular carcinogenesis (Allan Balmain). Building on his insight into the molecular genetics of cancer, Balmain led the research leading to the first clinical trial of an oncolytic virus which targeted cancer cells which lack functional p53 (Ganly et al 2000).
In 1986, the Glasgow team co-founded the Scottish Gynaecological Cancer Studies Group which went on to lead on several key national and international trials in ovarian cancer (Kaye et al 1992, 1996, Vasey et al 1999, 2004). From this base, and building on initial work by Stephen Merry, an increasing translational research interest in mechanisms underlying drug resistance developed, with valuable laboratory input from Bob Brown, Ian Freshney and Jane Plumb. This remains a key obstacle to progress in cancer therapy and the Glasgow team were the first to recognise the importance of tumour sample analysis (using tumour DNA in the circulation) in addressing these challenges (Gifford et al 2004).
In addition to the translational research programme linked to novel therapy, the Department retained a strong interest in patient-centred research, building on the foundations laid in the 1970s and early 1980s and involving support groups and expert psychology input.
The framework provided a fertile training ground for a number of individuals who went to fulfil senior professorial roles in Glasgow and elsewhere in the UK. These include David Kerr, David Cunningham, Will Steward, Chris Twelves, Duncan Jodrell, as well Jeff Evans.
Professor Cassidy left Glasgow in 2011 to work in the pharmaceutical industry. At that stage the Department was renamed “The Centre of Oncology and Applied Pharmacology”.
Professor Jim Cassidy
Images unless otherwise noted provided by authors
20th Century