


Our questions are:
Can we recommend better ways for social care and health services to work work together to help adoptive and foster families?
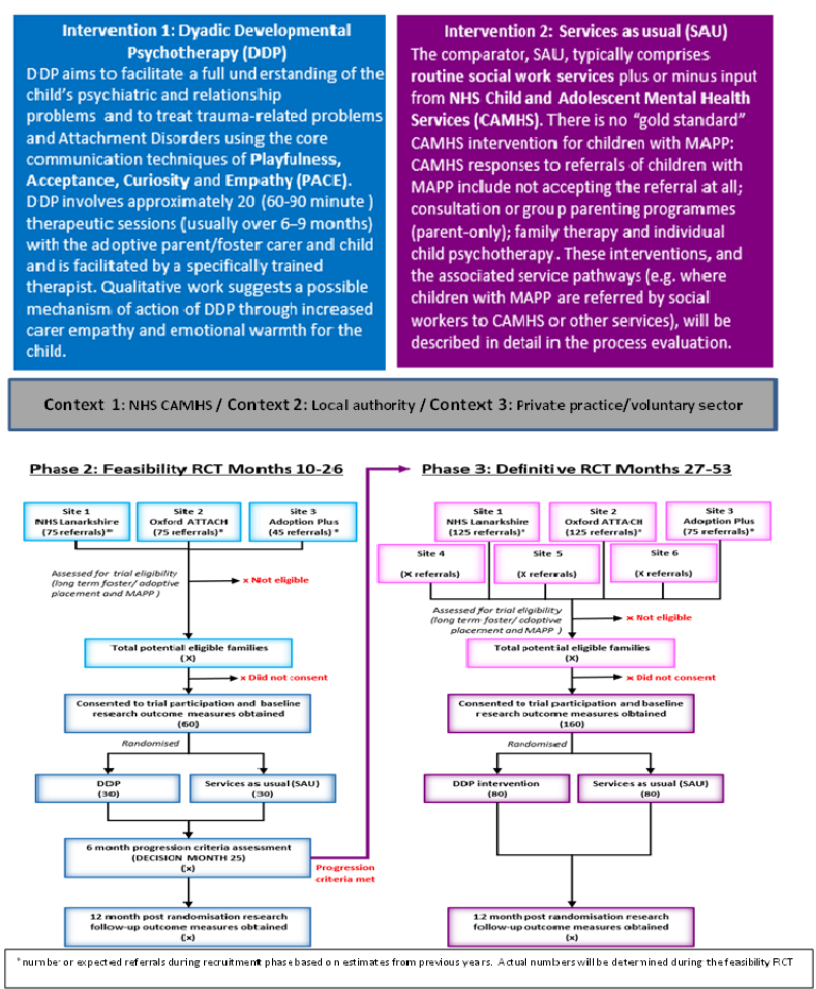
Can a therapy called DDP (Dyadic Developmental Psychotherapy) improve the mental health of 5-12 year old fostered or adopted children?
Is DDP worth the commitment families need to give to it - and the extra cost to the services that deliver it?
Why is this important?
Nearly all adopted or fostered children in the UK have been abused and neglected. More than half have mental health problems including ADHD (i.e. hyperactivity, impulsive behaviour and poor concentration), antisocial behaviour and problems with relationships. Abused and neglected children are more likely than others to have problems in school, become homeless, get involved in crime and even die young (e.g. from suicide), yet we have no fully tested treatments for their complex mental health problems. This is a huge problem because early treatment could greatly improve their life chances - and reduce strain on health and social care budgets. DDP is a parent-child therapy that takes around 20 sessions and focuses on “Playfulness, Acceptance, Curiosity and Empathy” (PACE). We don’t yet have really good evidence for or against it: many UK therapists like DDP, but it is a big commitment for families: once a week for about six months children will need time off school, their parents will need time off work - and this can be hard to explain to school friends, colleagues and bosses. We don’t just need to know if DDP improves children’s mental health – we also need to know if the commitment needed is worth it for families and whether the costs to services outweigh the benefits.
How do we plan to do this?
In PHASE 1 (9 months) we will find out whether DDP can work smoothly in the three different settings where it is usually delivered: the NHS, Social Care and Private Practice. Many abused children need other medical and psychiatric support so, before including an area in the next phase of the study, we will assess whether children can get any additional assessments or referrals they might need. We will use in-depth interviews with therapists and service managers linked to DDP and usual services to make this judgement. COMPLETED
In PHASE 2 (17 months), we plan to find out if it is practically possible to run a high quality trial of DDP. This phase will involve 60 families to find out if they are happy to take part (whether offered DDP or usual services) and make sure everything works well. If all goes to plan, these 60 families will contribute to the final results, along with the 120 families involved in the next phase. COMPLETED
In PHASE 3 (27 months) we will test whether DDP is better than usual services and, if it is, whether the improvements in child mental health outweigh the costs. Adoptive parents, foster carers and young people who have been in care as well as Health and Social Care Commissioners have advised us and will continue to do so throughout the study.
Phase 1: Intervention/Context Optimisaiton Months 1-9
What impact will the research have?
NICE Guidelines say abused and neglected children need help from health AND social care but, in practice, families often bounce around services without getting what they need. This study will make recommendations about how services should work together to help abused and neglected children and their families. If we find that DDP is worth the time and money, it could improve the mental health of abused and neglected children across the world.