

Academic Lead: Prof. Mia Crampin 
Summary
Malawi Epidemiology and Intervention Research Unit (MEIRU), formerly known as Karonga Prevention Study has, over the last 30 years, made major contributions to the understanding and control of mycobacterial disease, HIV and other infectious diseases.
MEIRU currently has urban and rural study platforms in Lilongwe and Karonga, and includes a demographic surveillance site in rural Karonga.
MEIRU’s main focus from 1979-2012 was in the rural Karonga District in Northern Malawi and was at the forefront in undertaking the first leprosy surveys in 1972 and collecting the first HIV infected blood spots in Karonga in 1982.
The Karonga data set contains over 1,500,000 contacts with more than 320,000 individuals, fully linked. e.g. Epidemiological, Clinical, Immunological, Genetic, Typed pathogen linkages.
In 2012 MEIRU established an additional urban site in Lilongwe, and started a major programme of work on non-communicable diseases, specifically cardiovascular disease and diabetes, both in Karonga and Lilongwe, to complement its continuing research on infectious diseases.
The extension of MEIRU to include urban Lilongwe was driven by the necessity to conduct research, to international levels of excellence, on the management and prevention of high burden diseases in Malawi.
Lilongwe’s data has mirrored systems from field, laboratory, data linkage and identification number compatibility. Collectively there is Linkage to biorepository (detailed identifying and epidemiological data) for over 400,000 samples and TB isolates over 35 years, all retrievable.
The addition of the urban site in Lilongwe has also provided the opportunity for MEIRU to seek the involvement of relevant stakeholders such as local academia, policy makers, community and patient groups.Additionally, MEIRU continues to develop capacity of Malawians in research methods, through formal courses and on-the-job training.
This collaborative and progressive model has provided the platform to maximise the benefits from our research for the people of Malawi and has been predominantly funded via the longstanding relationship with the Wellcome Trust.
Prof. Amelia (Mia) Crampin, whom has lived in Malawi for many years, is the Director of MEIRU and has been an integral part of the Karonga research facility since 1997. Professor Crampin provides extensive professional and academic expertise, to oversee the scientific activities, laboratories and data management across the organisation.
She has published widely in the epidemiology of HIV and TB, however in line with the progression of MEIRU, current work explores chronic conditions in Malawi, including hypertension, diabetes, obesity and depression.
MEIRU continues to renew and re-enforce its many partnerships with the College of Medicine (Malawi), MOH (Malawi), LSHTM and the University of Glasgow amongst others and recognises the increasing importance surrounding collaborative and integrative policy relevant research.
Integrative policy relevant research is imperative to address Malawi health challenges and the inequalities that currently exist within healthcare systems both locally and globally.
MEIRU is leading the way in conducting international levels of excellence surrounding research in Sub Saharan African (SSA) populations.
In doing so MEIRU is addressing some of the aforementioned health inequalities and contributing to better short and long term physical and mental health and wellbeing outcomes for those individuals their families and communities.
Recent Projects
Partners and Funding Bodies

COVSERO | SARS-CoV-2 Immuno-epidemiology in Urban and Rural Cohorts in Malawi: Generating Evidence to Inform Regional Medium- and Long-term Decision-making

Academic leads:
Glasgow: Professor Mia Crampin, Dr Antonia Ho
Malawi: Dr Charles Mwansambo, Dr Annie Mwale, Prof Nyovani Madise, Prof Victor Mwapasa, Dr Tonney Nyirenda, Dr Abena Amoah
Funder: Wellcome Trust
Dates: 01/09/20-28/02/22
Summary

Utilising the longitudinal urban and rural cohorts established by the Malawi Epidemiology and Intervention Research Unit, and supported by international and national expertise, we will undertake population immunoepidemiological surveillance to understand the trends in exposure and transmission of SARS-CoV-2, risk factors for SARS-CoV-2 infection and severe disease, as well as the proportion of asymptomatic or pauci-symptomatic infection in the population to enable an accurate estimate of infection fatality rate. Furthermore, we will recruit individuals with evidence of past SARS-CoV-2 infection or have received COVID-19 vaccine to a nested cohort with 3-monthly sampling, to explore the magnitude and duration of antibody response and protective immunity in the Malawian population, and at the same time creating a biorepository for further in-depth virological and immunological studies.
Results/ Outputs:
Field activities and round four data collection is now complete and final results of this study will be shared and disseminated in due course.
However, the Public Health Institute of Malawi (PHIM) kindly provided permission to release and disseminate key preliminary findings of ‘PREVALENCE OF COVID–19 ANTIBODY RESPONSES IN KARONGA DISTRICT & LILONGWE AREA 25 from a general population sample’. Individuals were randomly sampled from high density areas of KHDSS in Dec’20-Jan’21 and from remoter areas of KHDSS, and Lilongwe Area 25 in Mar’21.
Early Finding Conclusions:
1.First wave of COVID-19 resulted in considerable, previously un-recognized, transmission levels in the rural district, seroprevalence~ 5-10%
2.Second wave of COVID-19 in early 2021, resulted in majority of urban sample and a substantial proportion of rural sample being infected; Seroprevalence~ 56 % and ~ 34 %.
3.Rapid test sensitivity of 70% and the potential waning of antibodies suggest real cumulative infection prevalence in the community higher. Higher proportion of IgMin Karonga suggests more recent wave. After initial sampling concluded, participants were sampled every 3 months for one year on the following:
- Tests for whether their blood can neutralise SARS-CoV-2 (the virus that causes COVID)
- Tests for persistence of antibody response
- T-cell studies
- Asymptomatic SARS-CoV-2 infection (nasal swab)
NB: Final Results of this study will be disseminated in due course.
Healthy Lives Malawi
Academic lead: Professor Mia Crampin
Co-academic leads: Prof Victor Mwapasa, Dr Charles Mwansambo, Dr Robert Stewart, Dr Effie Chipeta, Prof Moffat Nyirenda, Prof Deborah Lawlor, Prof Debby Bogaert, Dr Marko Kerac, Prof Iain McInnes
Funder: Wellcome Trust
Dates: 01/10/20-01/10/24
Summary
Malawi is amongst the least developed and poorest countries world-wide. Adults, and particularly children, in Malawi still experience a lot of infections and increasingly suffer long-term illness such as depression, high blood pressure, diabetes and lung disease.
Studies that explore the causes and consequences of long-term illness require long-term follow-up. This project will build on existing work in urban/rural Malawi communities including 110,000 people, to conduct repeat adult health surveys and to nest a birth-cohort of 8,000 families in those communities.
The two study communities are different; rural subsistence farming/fishing and rapidly-growing urban. This will allow us to study and understand how socioeconomic, psychological, biological, nutritional, and infectious factors affect families’ health and wellbeing and to explore the persistence of ill-health and associated challenges between generations. Blood and other samples will be stored for future research. The resource will be made widely available to researchers to ensure maximum public health impact.
The aim of the Healthy lives Malawi Project is to create an intergenerational longitudinal population study of chronic conditions in rural and urban Malawi, leveraging substantial existing research infrastructure, to address the lack of high-quality longitudinal-data on chronic conditions in low income sub-Saharan Africa (LI-SSA).
Our prospective cohort data will provide age-specific incidence and survival estimates for multiple chronic conditions, and improve understanding of determinants (socioeconomic, psychological, nutritional, microbial and inflammatory) of health-related trajectories over the life-course, from poor pregnancy outcomes to multimorbidity in adulthood. Understanding how early-life exposures interact with later-life factors to mediate disease risk will indicate when and how to intervene effectively.
Wellcome LPS support will enable;
- Longitudinal tracking of 110,000 urban/ rural individuals.
- Repeat biomarker and clinical assessments of chronic conditions.
- Establish novel, effective migrancy tracking within/between rural/urban settings.
- Recruit/follow 7,500 nested families (grandparents-parents-siblings-pregnancy-birth-cohort); pregnancy, early-life and intergenerational effects.
- Health facility linkage; low-cost longitudinal health-care/outcomes data.
This resource will be shared with the global research community to best-practice guidelines.
Results/ Outputs
HLM DSS/LTC recruitment ongoing.
Epidemiology of multimorbidity (MM) of physical and mental health conditions in a rural Malawian population: early findings from Long-Term Conditions Survey
We investigated the distribution and determinants of Multimorbidity (MM) within our rural study site using preliminary data from our ongoing Long Term Conditions (LTC) survey in Malawi. The results presented below are from a cross-sectional study which is nested within our rural and urban demographic surveillance system the HDSS, which plans to follow up approximately 110,000 individuals, while the cross-sectional survey on long term conditions only targets all adolescents and adults (i.e., individuals aged 15 years and above).
Data Collection
- Rural study initiated on October 19, 2021 onwards.
- Urban study to commence in July 2022.
- Interviewer-led questionnaires on prior diagnosis or treatment for physical and
- mental health conditions and socio-demographic and lifestyle risk factors
- Physical measurements include anthropometry, blood pressure and body
- composition
- Fasted venepuncture blood samples for blood glucose, full blood count and
- biomarker sub-studies
Measures
Using early data from the LTC survey, we extracted data on 10 physical and mental health LTCs (and their risk factors) including:
- High blood pressure/hypertension
- Diabetes
- Heart disease
- Stroke
- Chronic pain
- Disability
- Depression
- Anxiety
- Asthma
- HIV
A self-reported prior diagnosis or current treatment were used to define diabetes, hypertension, asthma, heart disease, stroke, and HIV and MM was defined as having ≥2 physical or mental health conditions.
Analysis
We investigated WHO standard population age standardized and age-sex specific prevalence estimates for LTCs and MM and Logistic regression models were used to examine the association of selected sociodemographic and lifestyle factors with MM.
Conclusion
Out of the 2024 approached individuals, 2002 were interviewed (99% response rate) and 460 (23%) were multimorbid. These early findings indicate that MM is high in Malawi and commences early in adult life (15-24 years) and a large proportion of the Malawi rural adult population are living with multiple chronic health conditions. Multimorbidity increased with age across all age groups and the burden of MM was higher in middle aged women (40-54) compared with middle aged men. Given the severely constrained health systems in rural Malawi, targeted prevention and treatment measures are needed.


Generation Malawi
Academic leads- Professor Andrew McIntosh – University Of Edinburgh; Professor Amelia Crampin – University of Glasgow
Co-academic leads: Prof Victor Mwapasa, Dr Effie Chipeta, Prof Moffat Nyirenda, Prof Deborah Lawlor, Prof Debby Bogaert, Dr Marko Kerac, Prof Iain McInnes, Dr Lucinda Manda-Taylor, Dr Luis Gadama, Dr Eric Umar, Dr Genesis Chorwe Sungani, Dr Elizabeth Chodzaza, Dr Emmie Mbale, Dr Melissa Gladstone, Dr Linda Nyondo Mipando, Dr Kazione Kulisewa, Dr Effie Chipeta, Dr Charles Mwansambo, Dr Deborah Nyirenda; Dr Robert C Stewart, Dr Angus Macbeth, Dr Martyn Pickersgill.
Funders: MRC GCRF and Wellcome Trust
Dates: 01/08/20-31/01/24
Summary
Generation Malawi is a joint UK Medical Research Council (MRC GCRF) and Wellcome funded longitudinal study of mental and physical health in families in Malawi.
The 5-year study is a collaboration between University of Edinburgh, University of Glasgow, Malawi Epidemiology and Intervention Research Unit (MEIRU), University of Malawi College of Medicine (COM) and Kamuzu College of Nursing (KCN), LSHTM, University of Liverpool and others.
Generation Malawi will establish a multi-generational family/birth cohort in the rural (Chilumba) and urban (Lilongwe Area 25) MEIRU research sites through which to study longitudinal course and pregnancy, early-life and intergenerational effects for chronic mental and physical health conditions.
Generation Malawi is part of a linked programme of longitudinal population studies of chronic health conditions in the MEIRU sites alongside the Healthy Lives Malawi studies: Health and Demographic Surveillance Sites (HDSS) and a cross-sectional chronic health conditions survey.
The Generation Malawi protocol, under development, will aim to recruit, 8000 pregnant women from antenatal clinics; baseline assessments will take place at the participants’ homes from where spouses and wider family members will also be recruited.
A battery of questionnaires will be used to identify common mental and physical health conditions and risk factors (e.g. household characteristics, IPV, adverse childhood experiences, social support, socio-economic status). Anthropometry, other physical health measures and, in the pregnant women, ultrasound pregnancy dating will be conducted.
In addition, biological samples will be taken. These will be stored for later genotyping in a biorepository that will be established by the project.
Participants will be followed up and repeat mental and physical health measures will be conducted. Infant birth outcomes, infant growth and neurodevelopment will be recorded along with measures of mother/child interaction.
DIPLOMATIC: Pre-Term Birth and Stillbirth
Chief Investigator: Professor Jane Norman
PI: Professor Amelia Crampin
Co-I’s:, Professor Rebecca Reynolds, Professor John Norrie
Funder: NIHR Global Health Research programme
Dates: 01/04/18-31/03/21
Summary
DIPLOMATIC: Using eviDence, Implementation science, and a clinical trial PLatform to Optimise MATernal and newborn health in lICs (Low Income Countries). The aim of DIPLOMATIC is to reduce preterm birth and stillbirth and to optimise outcomes for babies born preterm in Malawi and Zambia
DIPLOMATIC is a Global Health Research Group Based in the UK, Malawi and Zambia.
Our vision is to reduce mortality of children under 5 years (one of the targets of sustainable development goals) by reducing preterm birth and stillbirth and to optimise outcomes for babies born preterm.
Globally 15 million babies are born preterm each year and over 2.5 million are stillborn. Deaths from preterm birth complications are the main global cause of under-5 mortality, accounting for an estimated 1·055 million child deaths in 2015. Low and middle income countries bear the brunt of this burden. Annual deaths from preterm birth and stillbirth in Malawi and Zambia are over 36,500 and The World health Organisation has estimated that the majority are preventable
More specifically, this project aims to:
- Enhance clinical care strategies for the prevention of stillbirth and pre-term birth in Malawi and Zambia, reducing rates of preterm birth, stillbirth and under-5 deaths
- Generate new knowledge on the effectiveness of interventions and on how best to implement them
- Develop a clinical trials platform to test NOVEL INTERVENTIONS, initially for stillbirth and preterm birth, but longer term in an NIHR unit on maternal newborn global health
- Enhance the collection of perinatal outcomes in vital statistics and hospital datasets
- Increase the accuracy of prematurity estimates by using first trimester ultrasound scanning to optimise assessment of gestational age
We recognise the differences that cultures, traditions, gender roles, resources, workforce constraints, disease burdens and community understandings of pregnancy and birth bring, and have therefore designed this group to examine strategies to develop and implement contextualised, evidence based local practices building on successes and challenges of current best practice in the UK and other high income countries.
Together with partners, and using a consensus exercise, we will identify Evidence Based Practices (EBPs) from the recommendations from the World Health Organisation (WHO), other stakeholders and from regional expertise: for example kangaroo care for preterm newborns, antibiotics for women with preterm premature membrane rupture, first trimester ultrasound scanning to accurately determine gestation, and (where gestation is known) steroids for women likely to deliver preterm.
By sharing existing knowledge on evidence-based practices and implementing new trial designs, our aim is to see a significant improvement at the end of this three year study.
NoToNa: Tackling cardiovascular risk in the adolescent life-course through a schools' salt-reduction intervention in sub
Academic lead: Professor Amelia Crampin – University of Glasgow
Co-academic leads: Prof Frances Mair, Dr Jones Masiye, Dr Beatrice Mwagomba, Professor Emma Mcintosh, Dr Marko Kerac, Professor Judith Glynn, Professor James Carpenter
Funder: MRC
Dates: 01/05/18 -30/04/21
Summary:
High blood pressure, which can lead to strokes, heart disease and kidney disease, is an increasing problem in sub Saharan Africa, and starts young. Excessive salt intake is a major contributor to this.
In some countries salt intake has been tackled through regulation of the processed food industry, but in much of sub-Saharan Africa little processed food is eaten and most salt is added at home. In Malawi we already have evidence of worrying levels of high blood pressure in teenagers, and high salt consumption.
Working with the School Health and Nutrition Programme, we propose to conduct a trial of an intervention package in schools in rural and urban Malawi which aims to reduce salt consumption in adolescents and their families. Of 26 schools, half will be randomized to receive the intervention and half will receive the normal school curriculum.
The intervention will take place over one school term and will be delivered to children in Year 6. It will include lectures, discussions, homework including food diaries, competitions, drama and family quizzes. It is modelled on a successful intervention in China, and will be adapted for local use.
Aim
- We will measure the effect of the intervention by measuring salt excretion (in urine) and blood pressure in a random sample of 20 children per school and their parents/guardians.
- We will compare the change in measurements from baseline to end of the intervention in participants from intervention and control schools, and will measure again at one year to assess the persistence of any effects of behaviour change.
- We will also assess factors that have helped or hindered implementation of the intervention, and will measure cost-effectiveness.
This will be very important in deciding whether and how to scale up the intervention.
Results/ Outputs
POSTER PRESENTATION: Feasibility and acceptability of a primary school-based salt-reduction intervention in rural and urban Malawi

Background
Hypertension is the leading risk factor for cardiovascular diseases and a major cause of death globally. The World Health Organization recommends sodium intake <2g per day (equivalent to 5g of salt). However, Malawi has high discretionary salt intake with >50% households reporting over 5g of plain salt per day, most added during/after cooking making behaviour change crucial. This qualitative study describes findings relating to perceptions of our pilot trial, including identified challenges and facilitators likely to influence success of the full trial.
Materials and methods
Qualitative methods were used, and Data was analysed thematically via Normalization Process Theory under 4 pillars which covered 1) how participants made sense of the intervention 2) engagement work to ensure participation 3) putting the intervention in to practice, and 4) appraisal of the intervention.
Results
Making sense of the intervention (Coherence)
- Respondents appreciated the intervention importance, understood the harmful effects of excessive salt intake but had difficulties measuring the recommended daily intake (5g) and calculating daily salt intake for big families
- Learners shared their experiences with parents, extended families and neighbors.
- Parents/teachers felt parent meetings (part of the intervention) were informative and motivating (although not all engaged)
Relationship work (cognitive participation)
Doing the work of participating in the trial (collective action)
- Reducing salt intake was hard work/time consuming e.g. hiding salt shaker, growing spices
- Some parents did not want to take instruction from their children and there was resistance from relatives or visitors.
Perceived facilitators to intervention (reflexive monitoring)
- Perceptions that the reduced salt intake had improved their health
- Terminology used in learning materials was unfamiliar to learners and learners felt language made lessons difficult to understand
- Teachers said lessons took longer than planned and thus forced them to hold the learners beyond school hours
- Teachers reported inadequate teaching materials to fit big classes
Perceived challenges to intervention (reflexive monitoring)
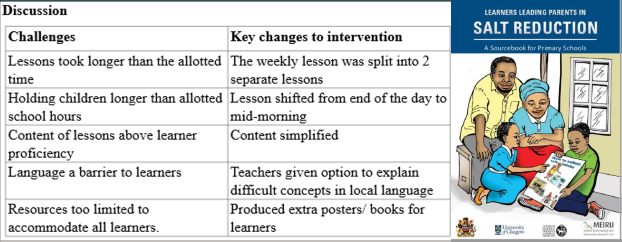
This qualitative research was received positively by participants and identified important barriers to successful uptake and integration of the intervention.
Leisure or Livelihoods? Youth Perspectives on Gambling and its Social, Economic and Health Impacts in Ghana and Malawi
Academic lead: Dr Darragh McGee – University of Bath
Co-Academic lead: Dr Christopher Bunn
Funder: British Academy
Dates: 20/03/20-19/12/21
Summary
This project adopts a participatory action research (PAR) approach to give voice to youth perspectives on the growth of commercial gambling across Sub-Saharan Africa (SSA), including its differentiated impacts on individual and community well-being.
Drawing on a comparative case study of Ghana and Malawi, as exemplars of, respectively, a mature and an emerging gambling market, the research aims to empower young people to convey the changing social and economic significance of gambling in their communities,including the extent to which technological advances have reshaped attitudes towards gambling practices,and how this may have wider implications for traditional conceptualisations of work, livelihood and social mobility.
The aim of this project is to create a paradigm shift in the ways in which we seek to understand and address commercial gambling across SSA.
Led by the voices, lived experiences, values and actions of young people, it proposes to reveal the differentiated socio-cultural, economic and technological significance of expanding gambling markets in Ghana and Malawi. In doing so, it could not be more timely.
Historical lessons from commercially mature gambling markets in the Global North suggest that research too often lagged behind the growth of the industry, and as a result, efforts towards intervention were stifled by strategic industry tactics.
And while gambling is increasingly acknowledged as a significant public health issue across SSA, the need for independent research and evidence of the everyday meaning, impacts and potential harms of commercial gambling has never been greater.
Culture and Bodies: an interdisciplinary approach to non-communicable disease prevention in Malawi and Tanzania
Academic lead: Prof. Cindy Gray – University of Glasgow
Funder: MRC/AHRC joint GCRF Scheme
Dates: 01/03/18 – 31/8/19
Summary
The incidence of non-communicable diseases such as hypertension and diabetes is rapidly increasing in countries in Sub- Saharan Africa, like Malawi and Tanzania. In 2010, there were more than 2 million deaths from non-communicable diseases in the region, which was a 46% increase from 1990.
Many people in Malawi and Tanzania, as elsewhere in Sub- Saharan Africa, are moving from rural areas into cities.Here, calorie-dense foods and drinks are easily accessible, and opportunities to be physically active reduced.
These factors, together with traditional cultural norms, such as a larger body size being associated with respect and attractiveness, contribute to increasing risk of non-communicable diseases in both countries.
People's understandings and responses to non-communicable diseases draw on biomedical, as well as traditional, knowledges; traditional healers, as well as medical doctors and nurses, are consulted in attempts to understand (and treat) the symptoms of non-communicable diseases.
If interventions to prevent non-communicable diseases in Sub-Saharan Africa are to be effective, it is essential they reflect not only Western experiences and biomedical accounts, but also local knowledges, perceptions and values.
However, as these local knowledges and values are often deeply-rooted and unspoken, traditional research methods, such as surveys and interviews, are often inadequate to describe them.
Community arts offer an alternative approach. They have great potential to allow researchers to access people's cultural, emotional and historical beliefs and practices, and then to work creatively together with local communities to develop non-communicable disease interventions that reflect these beliefs and practices.
In this project, we aim to develop an interdisciplinary partnership of medical and social science, and arts and humanities researchers, and local arts organisations in Malawi and Tanzania to learn together as we work closely with local communities to create culturally-relevant approaches to non-communicable disease prevention in Malawi and Tanzania.
We will do this using a variety of methods drawn from the different disciplines we represent. We will first analyse existing survey data from both countries, and conduct a review of previous arts-based health promotion initiatives in the region.
This information will inform pilot projects in Malawi and Tanzania working with people living in or near cities to use community arts to access local knowledges, perceptions and values, and to develop a culturally-relevant intervention activity.
By the end of the project, we will produce a framework describing ways of using community arts in non-communicable disease prevention. This will allow us to apply for more finding to test, refine and evaluate the framework in other settings in Malawi, Tanzania, throughout Sub-Saharan Africa, and beyond.
The project will allow partners to develop new interdisciplinary understandings and skills around gaining access to complex local knowledges, perceptions and values, and working closely with local people to develop innovative approaches to non- communicable disease prevention.
Participation in the project will build research skills capacity in the UK, Malawi and Tanzania. Local communities will benefit from involvement in the project through becoming more aware of how to prevent non-communicable diseases in ways that are culturally-relevant for them.
We will publicise our findings widely to local residents, and to local, national and international policymakers, practitioners and other researchers, through face-to-face and online events, and conferences, and through local, national and social media.
We will also have a dedicated project website which will host project news and outputs (translated into local languages, where appropriate), as well as an online resource bank to support other researchers to use similar approaches to non-communicable disease prevention.
Co-developing a health and well-being programme for men who support Malawian football teams, with a focus on preventing non-communicable diseases
Academic lead: Dr Christopher Bunn – University of Glasgow
Dates: 1/10/18-30/9/19
Funder: SFC GCRF (Internal Competition)
Summary
Non-Communicable Diseases are a growing problem in Malawi. Domestic football is popular, and our lead partner, the Football Association of Malawi, has an existing health-promotion agenda.
We will collaborate with practitioners and researchers to co-develop, deliver and feasibility test an NCD prevention programme for at-risk men through Malawi’s football clubs.
Development of nutritional strategies for diabetes prevention in Malawian adults at high diabetes risk
Academic lead: Prof. Jason Gill
Dates: 1/3/18-30/6/19
Funder: MRC
Summary
In Malawi (and wider SSA) diabetes is exerting an increasing public health burden, with age-standardised death rates 5 times higher than high-income countries (HIC). This risks overburdening fragile health systems and has important economic consequences.
The Malawian diabetes phenotype differs from that seen in HIC, occurring at lower BMI and high despite high physical activity (PA). Thus standard diabetes prevention interventions of weight loss and increased PA are unlikely to be effective.
It is vital to develop effective diabetes prevention strategies for the Malawian context. Low muscle mass/strength and chronic inflammation are both strongly linked to increased risk of diabetes, and are likely important contributors to diabetes risk in Malawi, where muscle mass/strength are low and exposure to infection/inflammation is high.
Thus nutritional strategies to increase muscle mass and reduce systemic inflammation, by increasing protein intake and reducing the inflammatory potential of the diet, may be effective for diabetes prevention in Malawi.
Our long-term aim is to develop and implement effective and pragmatic large-scale nutritional interventions to prevent diabetes in Malawi.
The current phase of our work adopts the 6SQuID approach to begin developing new nutritional diabetes prevention intervention(s) as follows:
1) assessing links between nutritional intake/status, and physical/metabolic/inflammatory phenotype in Malawian adults at high diabetes risk
2) assessing nutritional practices and diabetes knowledge in Malawian adults at high diabetes risk to identify areas amenable to change
3) working with a key stakeholder network to develop potential theories of changes and identify how nutritional interventions may be delivered in Malawi.
In future proposals we will finalise intervention development and test feasibility, acceptability, short-term effectiveness; before ultimately undertake robust, long term evaluations of the most promising intervention(s).
MAfricaEE: Multimorbidity in Africa – Increasing Understanding of the Patient Experience and Epidemiology
Project Summary:
This project aims to address key evidence gaps in multimorbidity research in LMICs, that have been identified by the Academy of Medical Sciences, namely to enhance our understanding of "disease clustering in defined populations/patient groups" and "the experiences and preferences of patients with different types of multimorbidity". This project will involve 3 work-packages (WPs) and use data sources from 3 African nations, Gambia, Uganda and Malawi. These three countries are on the Development Assistance Committee (DAC) list of "least developed countries."
The work represents a collaboration led by the University of Glasgow (UoG), which has particular expertise in multimorbidity research, using both data science and qualitative methods, along with partners in Malawi, the MRC Units in Gambia and Uganda and the London School of Hygiene and Tropical Medicine.
Aims
The planned collaboration aims to build mixed methods research capacity in multimorbidity in Africa and the UK with the following objectives:
1. To explore available data sets in Malawi, Gambia and Uganda to identify and compare the prevalence and patterns of multimorbidity, including both physical and mental health conditions.
2. To use qualitative methods to explore the lived experiences of multimorbidity, with a particular focus on the concept of Treatment Burden.
3. To build institutional mixed methods research capacity, preparing a new generation of investigators in the partner institutions with an enhanced understanding of Multimorbidity and its implications in different contexts
4. To convene a forum of investigators from Malawi, Uganda, Gambia and the UK along with key stakeholders to share experiences of multimorbidity research, opportunities and key challenges
The project will promote mixed methods collaborative work in the sphere of multimorbidity in Sub Saharan Africa (SSA) that will underpin future research into the patient experience, the design of health and social care systems, the epidemiology and economics of multimorbidity in SSA as well as underpinning mechanistic work.
Project details:
Academic lead: Professor Francis Mair – University of Glasgow
UoG co-applicants: Dr. Chris Bunn, Professor Mia Crampin, Dr. Bhautesh Jani
Malawi Co-applicants: Dr. Gertrude Chapotera
Funder: Medical Research Council (MRC)
Start Date: 1st September 2020
End Date: 30th September 2022
Results/ Outputs
RESEARCH ARTICLE
Experiences of multimorbidity in urban and rural Malawi: An interview study of burdens of treatment and lack of treatment
Edith F. Chikumbu, Christopher BunnI, Stephen Kasenda, Albert Dube, Enita Phiri-Makwakwa1, Bhautesh D. Jani, Modu Jobe, Sally Wyke, Janet Seeley, Amelia C. Crampin, Frances S. Mair, on behalf of the MAfricaEE Project
https://doi.org/10.1371/journal.pgph.0000139
We explored: 1) experiences of men and women living with multimorbidity in urban and rural Malawi including their experiences of burden of treatment and 2) examined the utility of Normalization Process Theory (NPT) and Burden of Treatment Theory (BOTT) for structuring analytical accounts of these experiences.
Key elements of burden of treatment included: coming to terms with and gaining an understanding of life with multimorbidity; dealing with resulting disruptions to family life; the work of seeking family and community support; navigating healthcare systems; coping with lack of continuity of care; enacting self-management advice; negotiating medical advice; appraising treatments; and importantly, dealing with the burden of lack of treatments/services. Poverty and inadequate healthcare provision constrained capacity to deal with treatment burden while supportive social and community networks were important enabling features.
Greater access to health information/education would lessen treatment burden as would better resourced healthcare systems and improved standards of living. Our work demonstrates the utility of NPT and BOTT for aiding conceptualisation of treatment burden issues in LMICs but our findings highlight that ‘lack’ of access to treatments or services is an important additional burden which must be integrated in accounts of treatment burden in LMICs.
Enhancing connectivity and communications between Malawi Epidemiology and Intervention Research Unit and University of Glasgow
Project Summary: Due to in-country and international travel restrictions imposed by the COVID-19 pandemic, virtual communication became vital for collaborations between MEIRU and University of Glasgow (UoG). We improved the IT infrastructure and internet connectivity at the two MEIRU research sites by i) expanding video conferencing facilities, ii) installing fibre broadband and iii) configuring Virtual Private Networks. With ongoing travel restrictions, these additions improved delivery of MEIRU research activities by enabling more effective communication within Malawi, the UoG and other external partners.
Objectives:
It also facilitated bidirectional capacity building through remote training, joint seminars/workshops and enhanced data sharing.
|
Despite the challenges faced because of the pandemic and therefore global shortages of component parts of IT equipment and escalating international shipping costs, we are very proud to say that all of the above objectives were achieved and within budget!
Project details:
Academic lead: Dr Antonia Ho
UoG co-applicants:
|
Name |
School/Institute |
|
ECR? (y/n) |
|
Prof Amelia (Mia) Crampin |
IHW, University of Glasgow |
N |
|
|
Baltazar Bananga Mtenga |
IHW, University of Glasgow |
N |
|
|
Victoria Ferguson |
IHW, University of Glasgow |
N |
Malawi Co-applicants:
|
Mabvuto Luhanga (IT Manager) |
MEIRU |
Malawi |
Non-Academic |
|
Laurence Tembo (Finance Manager) |
MEIRU |
Malawi |
Non-Academic |
|
Abena Amoah (Science Manager) |
MEIRU |
Malawi |
Academic |
|
Stephen Kasenda (COVID study lead) |
MEIRU |
Malawi |
Academic |
Funder: Scottish Funding Council (SFC) & Global Challenges Research Fund (GCRF)
Start Date: 1st July 2021
End Date: 30th November 2021
Results/ Outputs
|
Output/Impact |
Mechanisms and Metrics that were used to determine if output/impact was achieved. |
|
Install videoconferencing equipment in MEIRU meeting rooms & laboratories |
1 meeting room and 2 laboratories are now equipped with videoconferencing facilities |
|
Install fibre optic backbone for better internet connectivity |
Internet speed has improved from 6 to 10 mbps at both Chilumba and Lilongwe sites. |
|
Install VPN between rural and urban sites |
Two VPN connections have been installed. |
|
Implementation |
Project reports on trainings, workshops and seminars conducted relating to joint MEIRU/UoG studies.
|
|
Societal Impact
|
|
|
The restrictions in travel and gatherings due to the COVID-19 pandemic meant that a significant proportion of research interactions needed to take place virtually, rather than in person. This was challenging for a research organisation in a low-income setting that’s based at two sites, with multiple research collaborations with overseas partners! IT infrastructure was urgently in need of upgrade.
This project improved ease of communication between MEIRU sites, and also between MEIRU and research partners outside of Malawi. The additional videoconferencing capability and improvement in internet speed also facilitated virtual training and therefore ensured smooth delivery of research studies during the pandemic.
|
|
|
|
The improved infrastructure continues to facilitate ongoing workshops, meetings and trainings related to existing projects, and makes the planning and implementation of future projects more feasible, extending the important work of MEIRU (particularly in collaborations with UoG).
|
|
|
There are approximately 200 staff across the MEIRU sites (research, research support and technical) who are benefiting from the improved internet for communication, work practices and training opportunities.
There are 10 laboratory staff across the two MEIRU sites who now have access to videoconferencing for training and updates at the bench. There are 80 research staff at the rural Karonga site who are benefitting from the videoconferencing equipment now installed in the meeting room, assisting in training and professional development.
This project has also enhanced our abilities to conduct interviews for new staff remotely and has been used in 4 recruitment opportunities to date |