

 Translational Cancer Pathology
Translational Cancer Pathology
My key research interests include the investigation of signal transduction mechanisms associated with the development and progression of breast, coloretal, renal and prostate cancer. My main aim is to identify clinically relevant aberrations in the human solid tumours and establish if they can be employed in clinical practise to improve patient care and outcome. This approach has confirmed members of the Src family, PI3K pathway, IKKs and MAPK pathway as potential therapeutic targets. In parallel to the clinical investigations, target validation is also performed in cell studies to establish the functional significance and relevance of activating and inhibiting these targets. Further details canbe found below.
Prostate Cancer
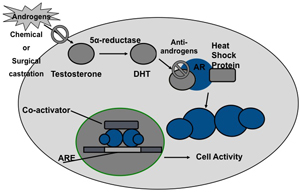 One of the many challenges in the effective management of prostate cancer is the identification of molecular markers capable of predicting disease progression. Many men are diagnosed with locally advanced and metastatic disease, which is treated by androgen ablation (including maximum androgen blockade). This treatment controls prostate cancer growth by hormonal manipulation, which inhibits androgen production or action on the androgen receptor (AR). Inhibition of testicular androgen production may be achieved chemically using agonistic/antagonistic agents against luteinising hormone-releasing hormone or surgically by orchidectomy. The action of androgen at the peripheral level is blocked by anti-androgens. Both forms of therapy have proven efficacy for different states of the disease.
One of the many challenges in the effective management of prostate cancer is the identification of molecular markers capable of predicting disease progression. Many men are diagnosed with locally advanced and metastatic disease, which is treated by androgen ablation (including maximum androgen blockade). This treatment controls prostate cancer growth by hormonal manipulation, which inhibits androgen production or action on the androgen receptor (AR). Inhibition of testicular androgen production may be achieved chemically using agonistic/antagonistic agents against luteinising hormone-releasing hormone or surgically by orchidectomy. The action of androgen at the peripheral level is blocked by anti-androgens. Both forms of therapy have proven efficacy for different states of the disease.
Although this approach has initial response rates of over 80%, the majority of men will eventually relapse with castrate resistant prostate cancer (CRPC). CRPC represents the lethal phenotype of prostate cancer and unfortunately is a common clinical problem, with a median survival time of 18-24 months. Until recently the only treatment to show any survival benefit following development of CRPC, was docetaxel chemotherapy. However, docetaxel only delays progression by a few months, meaning that more effective therapies are essential, as currently over 12,000 UK men die of this disease every year.
Recent advances have led to the approval of new hormonal agents with differing mechanisms of action. Results from clinical trials with the androgen synthesis inhibitor Abiraterone and androgen receptor antagonist Enzalutamide have provided evidence that CRPC remains androgen responsive. In Scotland on 13 August 2012, the Scottish Medicines Consortium (SMC) recommended that Abiraterone should be available within the NHS for men who have advanced prostate cancer, following failed first line hormone therapy and docetaxel. Similarly Enzalutamide was approved for use in Scotland on 8th November 2013, again this is only recommended as second line hormonal therapy after failure of docetaxel. Although none of these new treatments are considered curative (underpinning the need for new therapies), it is hoped that they will significantly extend CRPC patients survival. The challenge is therefore to identify biomarkers to predict which CRPC patients are most likely to respond and benefit from these new AR targeting drugs and identify novel modes of targeting the AR.
We have reported that AR amplification and an increase in AR protein expression are associated with development of CRPC and poor patient outcome. We also observed that those patients with AR amplification developed resistance to first line hormone therapy significantly faster than those who did not acquire this genetic aberration.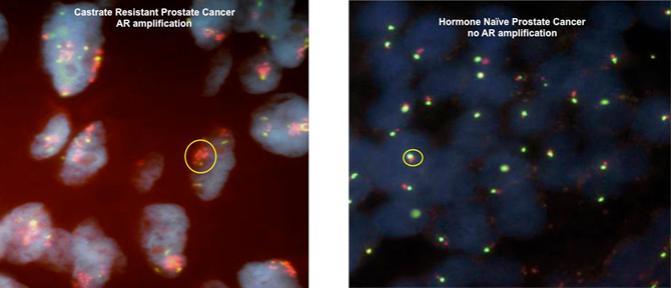
In addition to AR amplification and an increase in protein expression we have also investigated if phosphorylation of the AR could be employed as predicative biomarkers for prostate cancer. Upon binding of androgens, the AR undergoes phosphorylation predominantly at serine residues. We have established that phosphorylation at specific serine residues on the AR have differing roles in prostate cancer progression and the development of castrate resistant disease. In 2013 we reported that the AR is phosphorylated in response to DHT at serine 81 (AR81) and phosphorylation at this site is associated with phosphorylation of Cdk1 and an increase in tumour proliferation index. Inhibition of Cdk1 phosphorylation inhibits both DHT induced phosphorylation of AR at serine 81 and also tumour proliferation index. We predict that AR phosphorylation as a marker of progression to CRPC may define which men could benefit from Abiraterone following first line hormone failure.
In addition, over that past decade we have also gathered evidence that expression and activation of components of the PI3K cascade are associated with poor clinical outcome in castrate resistant prostate cancer via phosphorylation of the AR. We first demonstrated that PI3KCa was amplified in prostate cancer in 2003 and then observed that PTEN loss and AKT activation was associated with shorter patient survival and phosphorylation of AR at serine 213 (AR213) in 2008.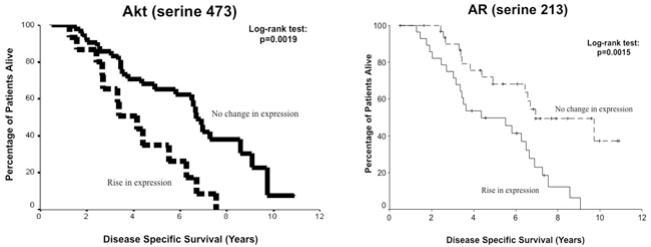
This is one possible mechanism allowing development of CRPC in the clinical setting and targeting PI3K cascade is a novel mode of treatment for CRPC. In addition to the correlations we observe with the PI3K cascade and AR213 in the clinical CRPC, we observe that silencing of PI3K inhibits EGF induced phosphorylation of AR at serine 213 but not serine 81, providing additional evidence that the PI3K cascade induces phosphorylation of AR at serine 213. Therefore patients with phosphorylation of AR at this site may be more likely to respond to inhibition of the PI3K pathway.
Our results to date lead us to hypothesise that AR amplification could predict response to AR antagonists eg Enzalutamide, AR phosphorylation at serine 81 could predict response to androgen synthesis inhibitors eg Abiraterone and AR phosphorylation at serine 213 could predict response to PI3K inhibitors eg BKM120. In addition we hypothesise that there is synergy between AR signalling and PI3K pathways, therefore dual targeting may benefit patients exhibiting this expression profile. The aim in the lab currently is to explore these mechanisms in more detail and provide evidence to support our hypothesis, with the eventual aim of developing clinically relevant biomarkers to aid the urologist in their clinical decision-making.
For further information on this area of the Edwards team research please contact Dr Joanne Edwards or Dr Pamela McCall.
Breast Cancer
Breast cancer is the most commonly diagnosed female cancer in the UK, currently there are over 45,000 newly diagnosed cases and over 10,000 breast cancer deaths each year. Around 75% of breast cancer patients are oestrogen receptor alpha (ER) positive at diagnosis. The ER is a nuclear receptor transcription factor, which is activated upon oestrogen (E2) binding, to regulate downstream oestrogen dependent genes, resulting in an increase in cellular proliferation and decrease in cell death. Current treatment aims to inhibit this by employing anti-estrogen therapies such as tamoxifen which competes with E2 to bind to ER and aromatase inhibitors (AI) which reduce circulating levels of E2. Although this therapeutic approach is successful for the majority of women, both de novo and acquired endocrine resistance remains a major clinical problem. To date the mechanisms underlying the development of endocrine resistance are poorly understood, and it has yet to be established if mechanisms underlying the development of tamoxifen and AI resistance are similar or a completely independent of each other. Approximately 30% of patients who recur whilst on Tamoxifen will respond to AIs, strongly suggesting that there are differences in the mechanisms associated with resistance to both these therapeutic approaches. Currently we are unable to predict if a patient will respond or develop resistance to either type of endocrine therapy and Gap analyses by the Breast Cancer Campaign in both 2008 and 2013 state a better understanding of mechanisms driving endocrine resistance is required (Thompson et al 2008, Eccles et al 2013).
In mammals, the NFκB family of proteins collectively is comprised of five transcription factors: p65 (RelA), RelB, c-Rel, p50/p105 (NFκB1), and p52/p100 (NFκB2). The activity of NFκB factors is tightly regulated at multiple levels; a) the inhibitors of κβ (Iκβ), b) the upstream kinases that phosphorylate Iκβs known as the Iκβ kinases (IKKs), and c) post-translational modifications that can modulate the Iκβ sand IKKs as well as the NFκB subunits themselves. We are interested in the primary level of regulation of NFκB pathway, namely the IKKs due to their key role upstream of the NFκB transcriptional machinery. There are two well-defined and distinct pathways that can lead to transcriptional activation of NFκB members via the IKKs: a) the canonical pathway where an IKK heterodimer (complex) consisting of two catalytic subunits IKKα and IKKβ, and a regulatory subunit IKKγ/NEMO is required for activation of the proto-typical p65/p50-Iκβα complex, and b) the non-canonical pathway where only IKKα is required for the proteolytic processing of p100/RelB dimer to p52/RelB. These NFκB pathways regulate the transcription of a wide range of genes involved in the immune response, inflammation, angiogenesis, proliferation and apoptosis. Many of these processes are hallmarks of cancer, therefore NFκB has been hypothesised to have a role in the development of tumour recurrence and disease specific mortality.
The non-canonical and canonical NFκB signalling pathways have been implicated in the development of hormone resistance in solid tumours. We have already reported that activation of the NFκB pathway is associated with poor outcome in prostate cancer patients in 2011) and is associated with progression to castrate resistant disease in 2012 and expression of NFκB has been reported to be elevated in breast cancer cell lines and in rat mammary tumours when compared to normal tissue. We therefore have been investigating the role of non-canonical and canonical NFκB pathways in the development and progression of breast cancer.
In a cohort of 544 breast cancer patients we have observed that nuclear expression of p-p65 S536 is a marker of activation for the canonical pathway, and is associated with significantly reduced disease free survival in ER positive disease but not ER negative disease. This is most evident in luminal B tumours and is associated with increased angiogenesis within the tumour as assessed by CD34. It was also observed that IKKα is a marker of activation of the non-canonical pathway and associated with significantly reduced disease free survival in ER positive disease. This was most evident and in luminal A tumours. Unlike p-p65 S536, IKKα expression was not associated angiogenesis but was associated with tumour size (p=0.028) and grade (p=0.018), cell death (apoptosis p=0.024, necrosis p=0.019) and inflammatory infiltrate within the tumour (Klintrup p=0.028). In addition, IKKα expression levels are also associated with quicker time to recurrence on Tamoxifen and again was most evident in luminal A tumours (p=0.00001).
We have also investigated the impact of siRNA of IKKα and IKKβ on ER positive MCF-7 breast cancer cells and ER negative MDA-MB-231 breast cancer cells. It was observed that in the MCF-7s, silencing of both IKKα and IKKβ significantly impact cell viability. In the MDA-MB-231 cells it was only silencing of IKKβ that had any impact on cell viability. and MDA-MB-231 (right) cell viability after siRNA treatment")
Our work to date suggests the NFκB pathways have diverging roles in ER positive breast cancer. The canonical pathway is associated with angiogenesis and recurrence in the luminal B subtype and the non-canonical is associated with reduced cell death (necrosis and apoptosis) and recurrence on tamoxifen in the luminal A subtype. Also we have evidence to support that intervening in these pathways influences cell growth and survival. We are currently working to validate these findings in an independent cohort and confirm by mechanistic studies.
For further information on this area of the Edwards team research please contact Dr Joanne Edwards or Lindsay Bennett